A patient with chronic kidney disease on dialysis
This is online E log book to discuss our patient’s de-identified health data shared after taking his/her/guardian’s signed informed consent. Here we discuss our individual patient’s problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problems with collective current best evidence based inputs. This e-log book also reflects my patient centered online learning portfolio and your valuable inputs on comment box is welcome .
Gnana Prasuna Reddy
Roll no. 49
Case:
65 year old man, who is a resident of nakrekal, a daily wage worker, came to the department with the chief complaints of high grade fever, cough with expectoration since 3 days.
Fever was continuous, associated with chills and rigors and subsided upon taking paracetamol medication.
Cough was associated with white coloured expectoration, which was scanty and increased during night times
It is not associated with any postural variation
He also complained of shortness of breath since 15 days.
According to the history, it is of grade 3.
There is mild pedal edema, of pitting type.
There are no complaints of decreased urine output, chest pain, palpitations, or any syncopal attacks.
Past history:
About 7 to 8 years back, followed by severe backache, this man developed high grade fever for which he was taken to a hospital in suryapet.
Upon further evaluation, his renal function tests were deranged, due to which he was diagnosed with renal failure at that time and was asked to get dialysis frequently along with some medications.
They later went to hyderabad for dialysis.
There, as they couldnt afford the cost, they started coming to this hospital for treatment since 5 years.
Initially he was only on medication, but gradually he was put on dialysis once a month.
Now he is getting dialysed once a week and for his fever, he is asked to come back for followup after 3 days.
He is not a known case of hypertension, tuberculosis, bronchial asthma, epilepsy, thyroid disorders
He is diagnosed denovo with type 2 diabetes mellitus 2 days ago
He does not have any history of previous surgical procedures.
Personal history:
Appetite is normal, diet is mixed, his bowel and bladder movements are regular, he has adequate amount of sleep and he smokes beedi occasionally.
Family history:
There are no similar complaints in any of his family members so far.
General examination:
Patient is conscious, coherent, cooperative, well oriented to time, place and person.
He is moderately built and moderately nourished.
There is no palor, icterus, cyanosis, clubbing, lymphadenopathy.
Pedal edema is seen, which is of pitting type and seen till the ankle level.
Vitals:
Pulse: rate: 106 bpm
Rhythm: regular
Character: normal
Volume: adequate
Condition of the vessel wall: soft
Delay: not seen
Blood pressure: 110/80 mm hg
Respiratory rate: 18 cycles per min
Temperature: 101 degree Fahrenheit
Systematic examination:
Cardiovascular system: both s1 and s2 are heard. No added sounds.
Respiratory system: bilateral air entry is present.
Central nervous system.: No focus neural deficits seen. Higher mental functions are intact.
Per abdomen: soft, non tender.
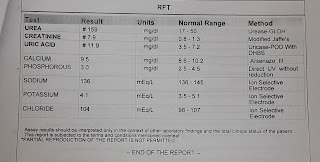
Provisional diagnosis: chronic kidney disease on hemodialysis.
Investigations:








Comments
Post a Comment